India is the second most unequal economy in the world after Russia, according to a 2017 Oxfam report entitled ‘An economy for the 99%.’ More sobering is the fact that even the people we might consider to be middle-class in India are really quite poor.
According to a study by Pew Research Center, even though India’s poverty rate fell from 35 percent in 2001 to 20 percent in 2011, the population that could be considered middle income saw only a marginal increase, going from about one percent to just three percent. This means that instead of a swelling middle class, India saw a movement of its population from poor to low-income* earners.
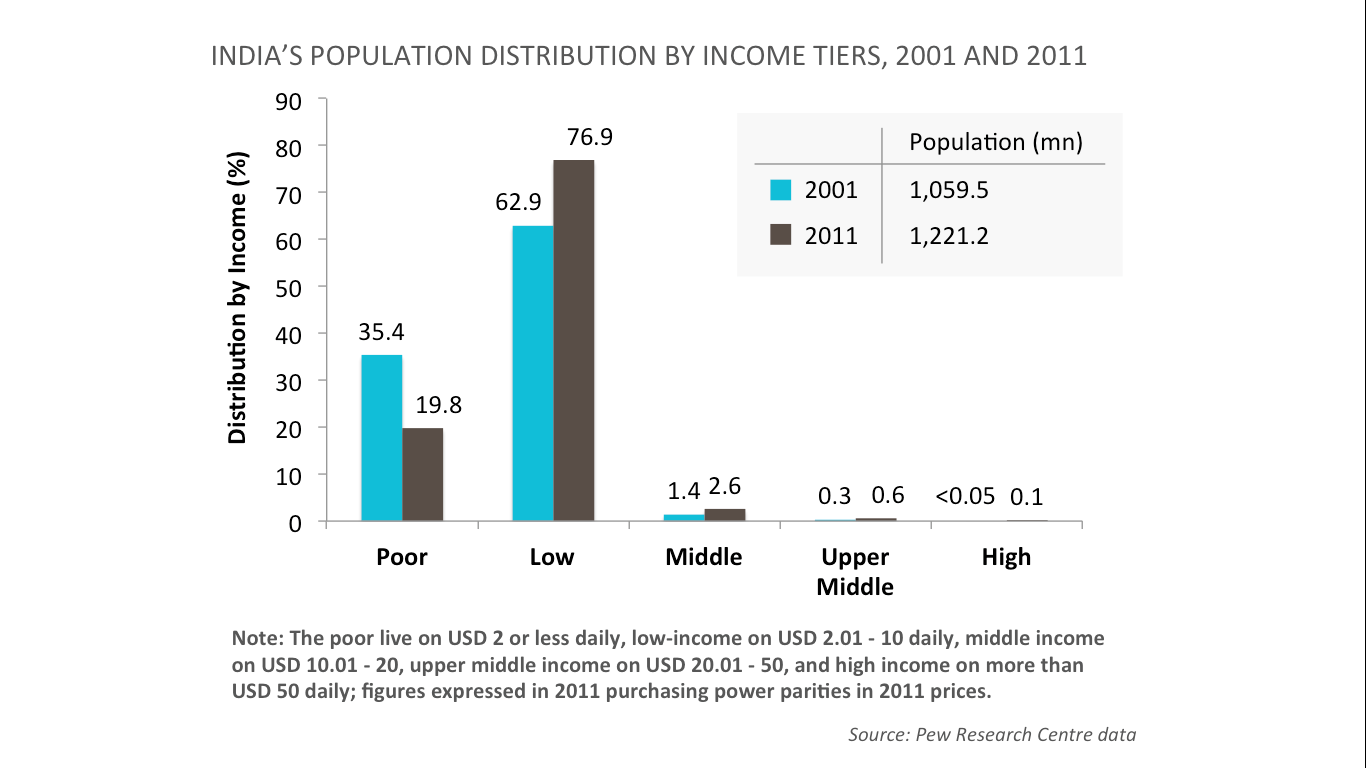
[quote]A large proportion of Indians are at the edge of the global poverty line–one economic or health shock away from slipping back into poverty.[/quote] The study pointed out that, “these were people hovering closer to $2 than $10 in daily income, and thus still a ways from the transition to middle-income status.” At that income threshold, a large proportion of Indians are at the edge of the global poverty line, possibly only one economic or health shock away from slipping back into poverty.
Where our efforts must lie
Given the sheer size of the problem, it would be infeasible for India to address this problem through transfers of wealth from the tiny sliver of high- and middle-income people (three percent of the population) to the poor and low-income (97 percent). The focus of the effort must instead lie in improving the environmental constraints that keep people in poverty and strengthening the enablers that can allow them to take charge of their own lives. Some of these enablers would include access to good healthcare and associated financial protection, basic financial services, good pre-school education and nutrition support services, and agricultural productivity services. However, strengthening these enablers, while eminently feasible, will not be easy.
Let us take healthcare for mothers and babies as an example
We know babies are more likely to survive when they receive essential newborn care–thermal care (drying and skin-to-skin contact), hygiene and infection control (cord-care and caregiver handwashing), and early and immediate breastfeeding.
We also know that these practices are more likely in clinical settings than at home in low resource settings. When these practices are followed diligently, women can return to their homes healthier and better able to take care of themselves and their babies. It also allows their children to thrive and to grow up into strong adults who are able to successfully pursue efforts that will change their income status. Ensuring that all of this happens has therefore become a key focus of efforts in the healthcare sector.

When new mothers are healthier and better able to take care of themselves and their babies, it allows their children to thrive and grow up into strong adults. (Photo courtesy: Charlotte Anderson)
An example of this is the Janani Suraksha Yojana (JSY), a government-run conditional cash transfer programme launched in 2005-06 to persuade women to deliver their babies in hospital settings. In the decade since it was launched, it has significantly improved the rate of hospital deliveries among rural women.
A nine-state analysis of the effects of JSY tells us the following: while inequality in access to care has reduced dramatically—in 2010, 49 percent of women on average were delivering at facilities, compared to 20 percent pre-programme—there still remains a large gap in accessing hospital-based delivery. The analysis reveals that nearly 70 percent of this could be attributed to differences in male literacy, disparities in access to emergency obstetric care and high levels of poverty.
In Bihar, for instance, after an initial spurt in women giving birth in facilities and delivery rates improving from 19.9 percent in 2005-06 to 63.8 percent in 2015-16, growth has stagnated in recent years. In some districts, such as Bhojpur, Buxar, Jehanabad, Munger, Patna and Rohtas, over 80 percent of women deliver in facilities, whereas in others, such as Darbhanga, East Champaran, Kishanganj and Sitamarhi, that figure is around 50 percent.
[quote]Despite India’s promising economic growth, 97 percent of the country would still be considered poor or low-income by global standards of poverty.[/quote]
A key finding from a recent study that examined the effect of Ananya–a health system training and community outreach intervention on reproductive, maternal and newborn health care utilisation in Bihar–was the large effect of gender inequity, specifically child marriage, on limiting the impact of the programme. We also know that maternal education and maternal incomes have strong positive associations with several health and development results including infant mortality, nutrition and women’s reproductive agency.
Efforts to further improve access to basic healthcare for mothers and babies, in addition to the JSY, would now need to address these additional sets of factors that research has revealed are acting as blockers to further progress.
Working towards an equitable India
India has made tremendous progress in reducing absolute poverty in the past two decades. The pace of poverty reduction has also accelerated over time: it was three times faster between 2005 and 2012 than in the previous decade. Despite this, and despite India’s promising economic growth, 97 percent of the country would still be considered poor or low-income by global standards of poverty.
Moreover, as we look beyond a monetary assessment of progress to other dimensions of well-being—nutrition, education, employment—we see that while those indicators have improved, they have done so to a lesser extent than in other developing countries.
For India’s future growth to be more equitable, as the healthcare example reveals, we will need to take into account myriad inter-connected and underlying factors. Fortunately, there are lessons that can be built upon, and in so doing, we can inch closer and closer towards an equitable India.
*Defined as between INR 34 and INR 170 per day, per person, or INR 170 to INR 850 per day, per family using a PPP exchange rate of INR 17 for $1.
With inputs from Amrita Agarwal, Debarshi Bhattacharya, Diva Dhar, Sabah Hamid and Suneeta Krishnan.
Views expressed in this article are personal.





